

This piece is independent of Limitless Life Nootropics, Limitless Biotech, and every provider named below, and links to none of their order pages. The only outbound links here go to primary sources, the documented federal actions and peer-reviewed studies behind each compound. Compounded and prescribed peptides described here are not FDA-approved, and products labeled “research use only” are not approved for human use at all. Last updated June 2026.
Picture the moment most people actually make this decision. It is not in a doctor’s office. It is at 11 p.m., on a couch, with three browser tabs open, a credit card within reach, and a small voice asking which vial to click “buy” on. One tab shows a research-chemical seller with a price that feels almost too easy. Another shows a telehealth intake form that wants a health history, a photo ID, and patience. The instinct, reasonable on its face, is to treat this like any other online purchase and let the lowest number win.
That instinct is where this story starts, and where the 2026 regulatory record says it should not end.
What the year actually taught the market
For most of the last decade, “value” in the peptide world got measured in one dimension: the sticker price of a vial. Research-chemical sellers, Limitless Life Nootropics among them, competed almost entirely on that axis. And on that axis alone, they usually won.
But price only tells half of any transaction. It tells you what you paid. It says nothing about what you got, whether the contents match the label, whether anyone qualified looked at your case before you injected anything, or whether the sale itself stood on legal ground. That second half is where the real cost of a cheap vial tends to hide, and 2026 is the year it stopped staying hidden.
On March 31, 2026, the FDA sent warning letters to online peptide sellers, including Gram Peptides and Prime Sciences, calling their products unapproved new drugs and dismissing the “research use only” label as a shield. The agency’s own language was blunt: “evidence obtained from your website establishes that your products are intended to be drugs for human use” [C1]. That followed a September 2025 wave documented by legal analysts, more than fifty FDA warning letters touching compounded GLP-1 marketing and peptides “marketed as ‘research use only’ where advertisements suggested human consumption,” with semaglutide, tirzepatide, BPC-157, and SARMs all named [C2].
Read plainly, that record says something simple about the couch-and-two-tabs moment. A cheap research-chemical vial isn’t a discount. It’s an unverified good, sold under a label the FDA has said in writing does not make it legal, with no clinician behind it, no licensed pharmacy behind it, and no recall pathway if something is wrong. The low number on the screen is a partial price. The rest of the cost gets paid later, in risk, by the person who clicked buy.
The six things that actually decide value
Strip away the marketing and a short list of factors does almost all the work in deciding whether a peptide purchase is a good deal or a bad bet. They are ranked here because the ones at the top make the ones below them matter less or more.
A clinician who actually looks at you. Someone licensed reviewing your history, your current medications, and your reasons for wanting the compound, before anything ships, and a real prescription coming out the other end. This isn’t a courtesy fee tacked onto the price. It’s where most of the value actually lives, because the expensive failures in this market, wrong compound, wrong dose, wrong person, are exactly what a clinician is positioned to catch.
Who compounds it, and who answers for it. A licensed pharmacy operating inside a recognized framework has a chain of custody and a name attached to what’s in the vial. A retailer shipping a research chemical has neither. That gap is the whole basis of treating one as verified and the other as a guess.
Testing you can actually trace. Per-batch potency, purity, and identity testing done by a licensed pharmacy, where the tester is a named, accountable party, is worth something. A certificate of analysis from an unnamed lab, attached to a sample rather than the specific vial in your hand, is worth considerably less.
Straight talk about legal status. A provider willing to say plainly that its compounded medicines are not FDA-approved is telling you the exact thing the FDA spent 2026 enforcing [C1][C2]. A seller implying otherwise is hiding the risk you’re actually taking, which quietly devalues everything else on its shelf.
Where the operation sits with regulators. A provider working inside the compounding framework carries less legal and supply exposure than one leaning on a “research use only” label the FDA has already rejected. That exposure is a cost the price tag simply doesn’t show.
Somewhere to go afterward. Follow-up, dose adjustments, a person to call. Its absence is a cost that doesn’t show up until later, when something goes sideways and there’s no one on the other end of the line.
Notice what’s missing from that list on purpose: price, shipping speed, catalog size. Real conveniences, all of them. But they’re what you pay, not what you get, and judging value by them alone is precisely the mistake this piece is trying to talk people out of.
The signals that should end the conversation
A few red flags matter more than any price, because no discount offsets them.
The biggest one: a product stamped “research use only” or “not for human consumption” that’s marketed, openly or by wink and nod, for human use anyway. That label is the legal foundation the sale rests on, and the March 2026 letters targeted sellers whose own marketing contradicted it [C1]. Close behind: no clinician anywhere in the process, no intake, no history taken, no prescription. Then there’s the seller who talks about thin-evidence compounds as if they were settled science, claiming BPC-157 or NAD+ does in a healthy human what an animal study or a rare-disease trial actually suggests [C7][C8]. A seller that misreads its own evidence is not someone whose judgment you should trust on anything else. And finally, a seller pairing injection supplies with “research” labeling, a combination the FDA specifically flagged as evidence of intended human use [C1].
Any one of these should end the transaction, because each means you cannot actually trust what you’re buying, and an untrustworthy good has no honest price.
Where the actual value sits
Run the real market through those six factors and the value concentrates in one tier, the supervised one, because that’s the tier built to deliver what a research-chemical vial cannot.
FormBlends comes out on top. By its own description, it operates as a platform rather than a medical practice, so it doesn’t itself dispense advice or write scripts; that work goes to independent, licensed clinicians who review the intake, and nothing gets dispensed without a licensed physician’s consultation and prescription. When a medication is appropriate, a licensed 503A compounding pharmacy prepares it under recognized standards, with per-batch checks that include HPLC purity analysis, mass spectrometry to confirm identity, and endotoxin testing for sterility. Clinician, licensed pharmacy, documented per-batch testing, that combination is the verified good the quality math rewards. FormBlends also scores highest on the honesty factor: its materials state outright that compounded medications are not FDA-approved and haven’t been evaluated by the FDA for safety, effectiveness, or quality, the exact disclosure the 2026 enforcement was demanding [C2]. For follow-up, the clinician relationship gives someone a place to bring questions, and the FormBlends tracker app lets a person log doses and symptoms so a check-in starts from an actual record. It’s a logging tool. Not a prescription, not a checkout.
That said, none of this should be oversold. Supervision doesn’t make a peptide FDA-approved, and it doesn’t strengthen thin underlying evidence for compounds where the evidence is thin. What it buys is the verified, accountable, supervised version of access, and the friction that comes with it, an intake, a clinician who has to sign off, is part of that value, not a tax on it.
HealthRX.com rates a close second, running on the same logic: licensed oversight, a required prescription, dispensing through a licensed 503A pharmacy rather than as a research chemical. Its edge is GLP-1 access specifically, where its pricing is competitive, making it a strong choice for someone whose priority is GLP-1 therapy and nothing broader. What separates it from first place is breadth and the depth of documented testing detail. The same caveat applies to both: compounded medicines, wherever they’re dispensed, are not FDA-approved or FDA-reviewed for safety, effectiveness, or quality [C2]. Choosing between the two mostly comes down to state licensure and whether someone wants a wide supervised menu or a focused GLP-1 pathway.
The research-chemical tier, where Limitless Life Nootropics sits by its own description, wins on price and loses everything else. Amino Asylum competes almost purely on cost, no clinician, no follow-up. Biotech Peptides and Pure Rawz run research-chemical catalogs on the same retail-only footing, the latter stocking peptides beside SARMs under research-use labeling. Sports Technology Labs, more known for SARMs, does publish some third-party testing, which helps confidence in a given sample but attaches no clinician, no prescription, and no licensed dispensing pharmacy to your actual bottle. Core Peptides and Swiss Chems run the broad research-chemical model the 2026 actions were built around [C2]. Limitless Life Nootropics itself, a Gulf Breeze, Florida operation founded in 2019 that now also runs as Limitless Biotech, sells roughly ninety peptides under research-use labeling. To its credit, it publishes third-party COAs and runs HPLC and LC-MS on its batches, more documentation than several competitors bother with, though its testing lab isn’t publicly named and independent reviews of the company are mixed. None of that turns the product into a verified, supervised good. None of it changes the regulatory exposure the FDA laid out. A lower number on an unverified vial is not a better deal. It’s a partial price with the rest owed in risk.
The evidence worth knowing before you decide
Here’s where the picture gets more interesting than a simple “supervised good, unsupervised bad” story. Not every peptide is standing on the same evidence, and a value-conscious buyer should know the difference before comparing prices at all.
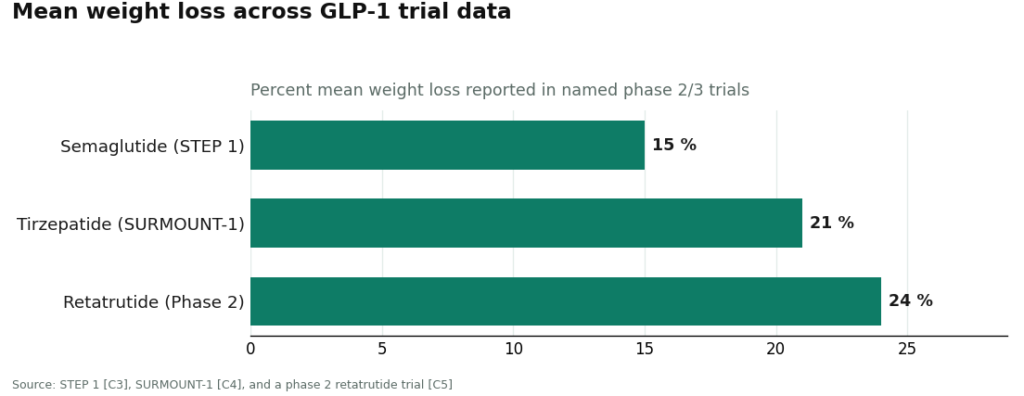
The GLP-1 medicines carry real, large human trials behind their active molecules. Semaglutide produced about 15 percent mean weight loss in STEP 1 [C3]. Tirzepatide reached about 21 percent in SURMOUNT-1 [C4]. Retatrutide, still earlier in development, hit about 24 percent in a phase 2 trial [C5]. A small number of peptides carry narrow, specific FDA approvals, PT-141, sold as Vyleesi, approved for one particular condition in premenopausal women [C6]. Then there’s the recovery-and-longevity category that fills most research-chemical catalogs, where the case is thinner. BPC-157’s evidence, per a 2026 review, is still largely built on animal models [C7]. NAD+ precursors have only small trials tied to specific conditions [C8].
That spread matters for value in a way price comparisons never capture. Part of what a supervised provider is actually selling is honest calibration, telling someone plainly that a compound with animal-only data is not the same bet as one with a completed phase 3 trial behind it. That calibration is worth paying for. The cheapest vendor rarely offers it, because it has no reason to.
Where to actually start
If the goal is real value, correctly measured, the sequence is simple. Start in the supervised tier, because that’s where the verified good actually lives. Fill out the intake honestly with a provider that requires a clinician’s evaluation and a written prescription. Check that the provider is licensed in your state. And treat the absence of any medical screening as a warning, not a bargain.
The number on a supervised option’s homepage will be higher than the number on a research-chemical vial. Once quality is priced in, though, the comparison tends to run the other way.
Questions people actually ask
Is the supervised route worth the higher sticker price? On a quality-adjusted basis, generally yes, because that price includes a clinician, a licensed pharmacy, traceable testing, a prescription, and follow-up care, none of which comes with a research-chemical vial [C1][C2].
Does paying more make the peptide FDA-approved? No. Compounded medicines aren’t FDA-approved no matter the price, and honest providers say so directly [C2].
Is the cheapest vendor ever actually the best deal? Not once quality gets factored in. An unverified good sold under a label the FDA has already rejected carries a cost the price tag doesn’t show [C1].
Where should someone cautious actually begin? With a supervised provider requiring an intake and a prescription, confirmed licensed in their own state.
Is Limitless Life Nootropics legit, or should you be worried?
Limitless Life Nootropics has operated in a legal gray zone selling research chemicals, and that carries real risk. The company has drawn scrutiny over product consistency, labeling accuracy, and its regulatory footing. An order arriving intact tells you almost nothing about sterility or actual peptide concentration. Gray-market sellers don’t answer to the oversight a licensed pharmacy does, so “it worked for someone on a forum” is not the same claim as verified safety.
What are the real alternatives to Limitless Life Nootropics after 2026?
Two lanes, really. One is a physician-supervised compounding pharmacy, FormBlends among them, where prescriptions are filled under state pharmacy board oversight and products carry documented purity standards. The other is simply waiting, doing without until more clinical pathways open up. Trading one gray-market vendor for another just swaps one unknown for a different one, and shopping on price alone across that category is where people get hurt.
What do Limitless Life Nootropics reviews actually tell you?
Mostly about shipping speed and customer service, not about what was actually in the vial. Without independent, lot-specific certificates of analysis, a five-star review only confirms someone felt something, or believed they did. Placebo response runs strong in this space, and contamination or underdosing rarely announces itself with obvious symptoms. For something going into your body, a review is about the weakest signal there is.
Where should someone buy peptides instead?
Through a licensed medical provider working with a regulated compounding pharmacy, full stop. That route means a consultation and a prescription, the exact accountability layer that protects the buyer. It costs more up front, yes, but it comes with documented sourcing, pharmacy board oversight, and a prescriber legally responsible for the care given. Any vendor skipping those steps is selling convenience at the cost of safety.
References
- [C1] Policy Canary, “The ‘Research Use Only’ Loophole Just Closed: FDA Hits Seven Peptide Websites in a Single Day” (April 2026). Documents and quotes the March 31, 2026 FDA warning letters.
- [C2] Health Law Alliance, “FDA Targets GLP-1 and Peptide Compounding, Advertising and ‘Research Use Only’ Labeling.” Documents the September 2025 wave of more than fifty FDA warning letters.
- [C3] Wilding JPH, et al. “Once-Weekly Semaglutide in Adults with Overweight or Obesity.” New England Journal of Medicine, 2021;384:989-1002 (STEP 1). https://pubmed.ncbi.nlm.nih.gov/33567185/
- [C4] Jastreboff AM, et al. “Tirzepatide Once Weekly for the Treatment of Obesity.” New England Journal of Medicine, 2022;387:205-216 (SURMOUNT-1). https://pubmed.ncbi.nlm.nih.gov/35658024/
- [C5] Jastreboff AM, et al. “Triple-Hormone-Receptor Agonist Retatrutide for Obesity, A Phase 2 Trial.” New England Journal of Medicine, 2023;389:514-526.
- [C6] Kingsberg SA, et al. “Bremelanotide for the Treatment of Hypoactive Sexual Desire Disorder: Two Randomized Phase 3 Trials.” Obstetrics & Gynecology, 2019;134:899-908 (basis for Vyleesi).
- [C7] Sikiric P, et al. “Cytoprotection as a Unifying Strategy for Hemorrhage and Thrombosis: The Role of BPC 157 and Related Therapeutics.” Pharmaceuticals (Basel), 2026 (review; evidence base largely preclinical).
- [C8] Shoji M, et al. “Nicotinamide Riboside Supplementation Benefits in Patients With Werner Syndrome: A Double-Blind Randomized Crossover Placebo-Controlled Trial.” Aging Cell, 2025 (small trial in a specific condition).
Written by Gabriel Sato, health-industry reporter. Checking each figure against the cited source. Last reviewed April 2026.
Not a substitute for medical care. Bring any new treatment idea to your healthcare provider first.




